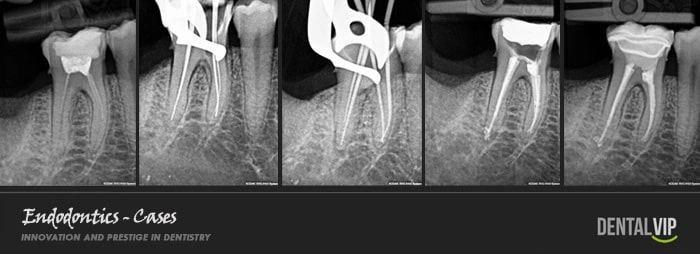
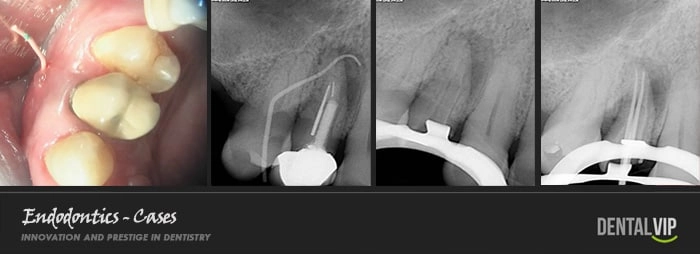
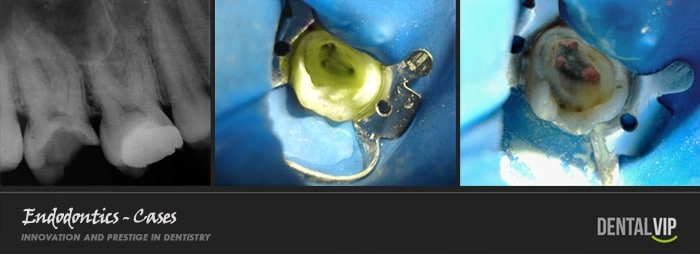
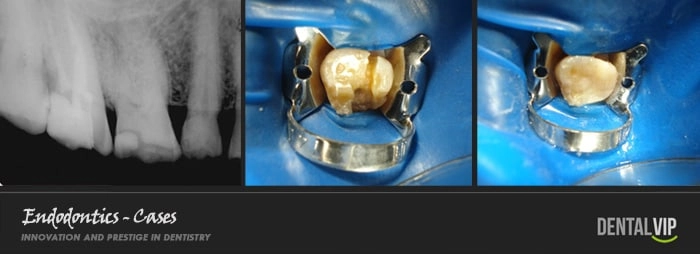
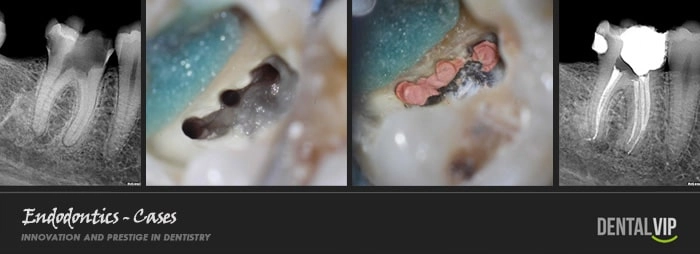
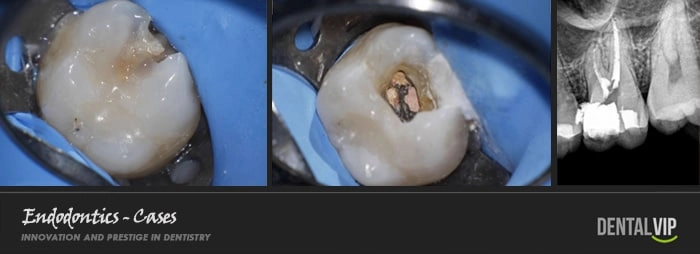
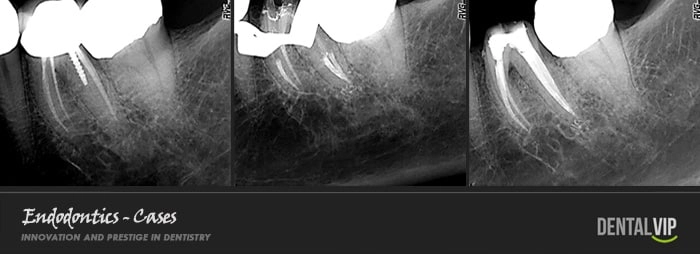
Any stimulus or aggressive entity capable of compromising the structural integrity of a tooth is also capable of causing damage, infection or necrosis of its pulp tissue. The dental pulp or "nerve" of a tooth is a specialized connective tissue that is lodged internally throughout the crown and root. When a trauma, excessive dental wear or indiscriminate advance of an untreated caries reaches, exposes or infects that pulp tissue, and of course we want to preserve the dental organ; there is no alternative but to remove it, disinfect and then mechanically widen the empty root canals so that they are capable of receiving an inert, sterile and biocompatible filling material that completely occupies them, avoids pain and the spread of the infectious process. In this consist a ROOT CANAL TREATMENT. If it is not performed on time, large facial abscesses, phlegmones or extremely painful and aggressive cellulite processes can be formed that can spread rapidly and seriously compromise other vital structures of the orofacial region, and in extreme cases; until the patient's life.
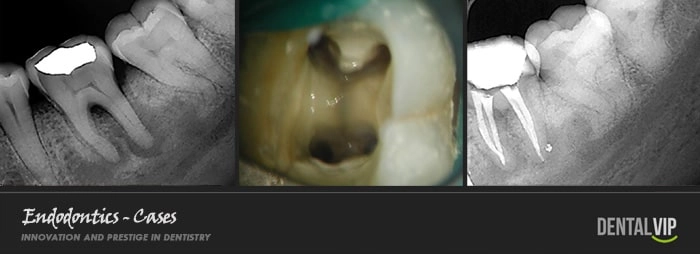
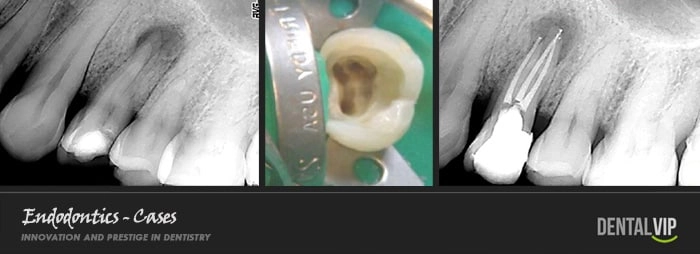
Given how intricate and variable the root anatomy of the teeth is and the fact that the canals are small cavities inaccessible to the human eye, it is a considerably hostile and difficult field of work, therefore it is necessary for the Dentist to have extensive anatomical knowledge of the RADICULAR MORPHOLOGY and has developed a very special sense of tactile perception that allows him to locate, access, instrument and fill the canals with great precision, with no margin of error possible. It is our opinion that such qualities are only achieved through formal studies of the Specialty and limiting professional practice exclusively to the area of Endodontics.
Our Endodontist has the latest technological advances such as high-speed rotary systems for mechanical canal instrumentation, electronic root apex locator, computerized digital radiology or RADIOVISIOGRAPHY that minimizes the emission of X-rays and modern thermoplastic shutter systems that reduce almost to zero the rates of clinical failure and the need for retreatments, periapical endodontic surgeries, apicectomies and dental extractions.